
Testosterone 101
TestosteroneAwareness
Testosterone is not a “male hormone”, it is a vital chemical messenger that supports energy, immunity, mood, metabolism, bone density, heart health, and brain function in both men and women. Understanding how it works is the first step toward reclaiming your vitality and long-term well-being.
Key Benefits of Healthy Testosterone Levels
- Cell growth and repair
- Bone and cardiovascular health
- Sugar and fat metabolism
- Muscle maintenance and red blood cell supply
- Immune regulation and reproductive support
- Neurological health such as balance, mood, mental health, and cognitive function
The Hidden Testosterone Crisis
- How everyday toxins from plastics to pesticides are silently lowering testosterone in both men and women
- How testosterone pellets, creams, and injections compare, and why steady delivery matters
- Uncover the myths about testosterone from heart disease to prostate cancer
Testosterone in Men’s & Women’s Health
- Cell Growth and Repair: Testosterone promotes the growth and repair of tissues, including muscle, nerve and bone tissues. It does this by stimulating protein synthesis, helping cells to repair and regenerate after injury or stress. This is necessary for the health of all tissues from liver to heart to blood vessels
- Bone Health: Testosterone helps to maintain bone density by regulating osteoblast activity (cells responsible for bone formation). This can prevent conditions like osteoporosis, which is more common when testosterone levels drop, especially in aging individuals. It does this by being the source for most all of the estrogen in your tissues, a critical tissue growth and repair hormone in both sexes.
- Cellular Metabolism: Testosterone affects the metabolism of fats, proteins, and carbohydrates within cells. It enhances the storage of muscle mass while encouraging the breakdown of fat and proper use of sugars, improving overall metabolic function and efficiency. It has been shown to improve diabetes while lessening falls and bone fractures.
- Red Blood Cell Production: Testosterone, through its one step conversion into estrogen, stimulates the production of erythropoietin, a hormone that increases the production of red blood cells in the bone marrow. Healthy red blood cells are essential for transporting oxygen throughout the body, supporting optimal cellular function.
- Immune System Support: Testosterone powerfully modulates immune function and inflammation. While its effects on immunity are complex and can vary depending on the individual, low testosterone levels are associated with increased susceptibility to infections. Testosterone balances immune responses, reducing the likelihood of both excessive or insufficient immune activity that is the basis of cancers, cholesterol plaques in blood vessels, and autoimmune diseases such as multiple sclerosis, Crohn’s disease, and fibromyalgia.
- Neuroprotective Effects: Testosterone has neuroprotective effects, meaning it supports brain health and cognitive function. It helps protect neurons from damage and promotes the regeneration of nerve cells, which benefits for overall neurological health.
- Influence on Cardiovascular Health: Testosterone powerfully affects vascular health by improving blood flow and influencing the activity of endothelial cells, which line blood vessels. Proper testosterone levels are linked to a lower risk of cardiovascular disease, while low levels may contribute to an increased risk of heart disease and strokes.
- Mood and Mental Health:Testosterone influences brain chemistry and mood regulation. Low testosterone levels have been associated with symptoms of depression, fatigue, and cognitive decline. Optimal levels are thought to contribute to a balanced mood, mental clarity, and overall well-being. Restoration of adequate testosterone levels in the tissues has been shown to reduce irritability, depression, anxiety, forgetfulness, and migraines.
Testosterone Therapy Options at a Glance
Comparing Creams, Injections, and Pellets for Effectiveness, Stability, and Health Impact
| Delivery Method | How It Works | Effectiveness | Controlled Release | Application Frequency | Common Issues | Type of Testosterone |
|---|---|---|---|---|---|---|
|
Pellet |
Small pellet inserted into a fat pocket under the skin
|
High |
Yes |
Quarterly |
Very few complications
|
Pure compressed human testosterone (derived from yam)
|
|
Cream |
Applied to skin |
Low |
No |
Daily |
Low absorption rate, inconsistent levels |
Synthetic testosterone |
|
Injection |
Injected into muscle |
Medium: T spikes up and down weekly
|
No |
Weekly |
Hormone spikes disrupt cellular estrogen balance |
Testosterone cypionate (requires enzyme activation) |
|
Pills |
Absorbed through digestive system |
Low |
No |
Daily |
Liver strain, hormone spikes if absorbed that disrupt cellular balance |
Synthetic undecanoate |
Myths About
TESTOSTERONE
False. Testosterone is the most abundant bioactive hormone in both men and women throughout their entire lives.
- Quantitatively, testosterone is the most abundant active sex steroid in women throughout the female lifespan, measured in nanograms/dl, which is 10-fold higher than the picograms/ml used for estradiol.
- It is the source of almost all the estrogen inside each cell in males and females. Serum estrogen is not transported across the cell membrane. Instead, testosterone is transported into our cells and some is converted into estrogen (a process called aromatization) within the cell itself, where it is critical to health and function of our tissues.
- From a biologic perspective, women and men are very similar, having both functional estrogen receptors (ERs) and functional androgen receptors (ARs). Testosterone, in balance with lower amounts of estradiol (E2), is equally important for health in both sexes.
- Functional androgen receptors are located in almost all tissues in the female body, including the breast, heart, brain, and bone, confirming its essential role far beyond any single gender association.
- German Women Primary Care Clinic studies found low testosterone women had the same large increases in deaths from all causes as did low testosterone men.
-
- Testosterone supplementation in deficient men reduces heart attacks, strokes, and cardiovascular deaths by over 50% compared to untreated men.
-
- Studies show testosterone therapy improves cardiac risk factors like fat mass, waist circumference, and insulin resistance.
-
- The initial studies suggesting cardiovascular risk were based on severely flawed methodologies and data errors, including the inclusion of women in an “all-male” study population.
-
- Decades of research show that testosterone causes most prostate cancer cells to die or regress, and no studies have shown it causes new prostate cancer.
-
- The false mythology about prostate cancer and testosterone was started due to a flagrantly poor study published in 1941 looking at one patient.
- The overwhelming weight of current scientific evidence shows no link between testosterone therapy and an increased risk or growth of prostate cancer.
-
- Androgen receptor (AR) signaling exerts a pro-apoptotic (promotes cell death), anti-estrogenic, growth-inhibiting effect in normal and cancerous breast tissue.
- Testosterone combined with an aromatase inhibitor is being used as a potential therapy for symptoms in breast cancer patients and survivors.
-
- Many safety concerns are mistakenly attributed to testosterone but are actually linked to oral synthetic steroids (which are liver-toxic) or to high estrogen levels that short term spikes in testosterone can sometimes create within the body. Modern, non-oral methods like pellets do not carry the same risks as older pill or injection forms.
-
- Testosterone therapy by pellet implantation has been proven as the only method to establish a long-lasting steady state supply of this critical hormone to men and women, used in the U.S. since 1940.
-
- Safety has been demonstrated even in long-term studies of transgender women to men using much higher doses, showing no increase in serious health problems like cancer or heart disease.
- 1930s: Testosterone pellets were first used in Europe and Australia, and compounded bioidentical hormone pellet therapy was developed to treat women who had undergone hysterectomies and remained in clinical use ever since.
- 1940s: Testosterone pellets were introduced in the United States and gained traction as a more stable alternative to oral hormone replacement therapies, which caused fluctuating hormone levels. Pellets were freely available to health providers.
- 1972: The FDA approved testosterone pellets at the request of a compounding pharmacy seeking a marketing advantage, but they were not consistently marketed in the US until 2008.
- 1970s–1980s: Their popularity declined in the U.S. as pharmaceutical companies introduced patented synthetic oral and topical hormone products.
- 1990s–2000s: Transdermal patches and gels were developed, becoming the preferred delivery methods for a time.
-
- The belief that it causes aggression stems from the misuse of high-dose, synthetic anabolic steroids, which is completely different from physiological testosterone replacement.
-
- In men and women, testosterone therapy decreased aggression and irritability in over 90% of patients treated for androgen deficiency symptoms.
- Research suggests that estrogen stimulation from synthetic anabolic steroids plays a leading role in aggressive behavior.
-
- At physiological replacement doses, testosterone stimulates femininity. Only very large doses used for gender “transitioning” can cause reversible side effects like increased facial hair or clitoral enlargement from engorgement.
- The unwanted side effects people worry about, like increased facial hair, are dose-dependent and reversible, and do not happen often. These side effects will fade if the dose is lowered, and many women find the benefits of treatment far outweigh these manageable side effects.
-
- Testosterone deficiency is actually listed as a potential cause of hoarseness, consistent with the hormone’s anti-inflammatory properties.
-
- Objective studies on women receiving testosterone therapy found no vocal changes attributable to the treatment.
- The idea that testosterone affects the voice comes from misinterpreted reports involving very high doses of strong synthetic steroids, not standard bio-identical testosterone treatment.
-
- Hair loss is complicated and is primarily influenced by genetics, hormones like dihydrotestosterone (DHT), and other factors like thyroid issues or iron deficiency.
-
- The belief that testosterone causes balding comes from confusing it with DHT, a different hormone that the body sometimes makes from testosterone.
- For many individuals, testosterone therapy can improve scalp hair growth. Research has shown that people treated with testosterone often see hair regrowth.
-
- Criticisms about inappropriate prescribing doesn’t reflect actual clinical practice or patient charts.
-
- The rise in prescriptions coincided with increased awareness of testosterone deficiency and reduced fear of prostate cancer, not pharmaceutical marketing, which is minimal for testosterone products since testosterone is a generic product.
- It’s illogical not to promote long-acting testosterone pellets for our national population as it is proven to reduce diabetes, cardiovascular diseases, cognitive and emotional problems, autoimmune conditions, bone and muscle loss, and more.
Understand Testosterone Level
Testosterone Decline Over the Years
Testosterone levels have had a substantial drop in the U.S. since the 1980’s.
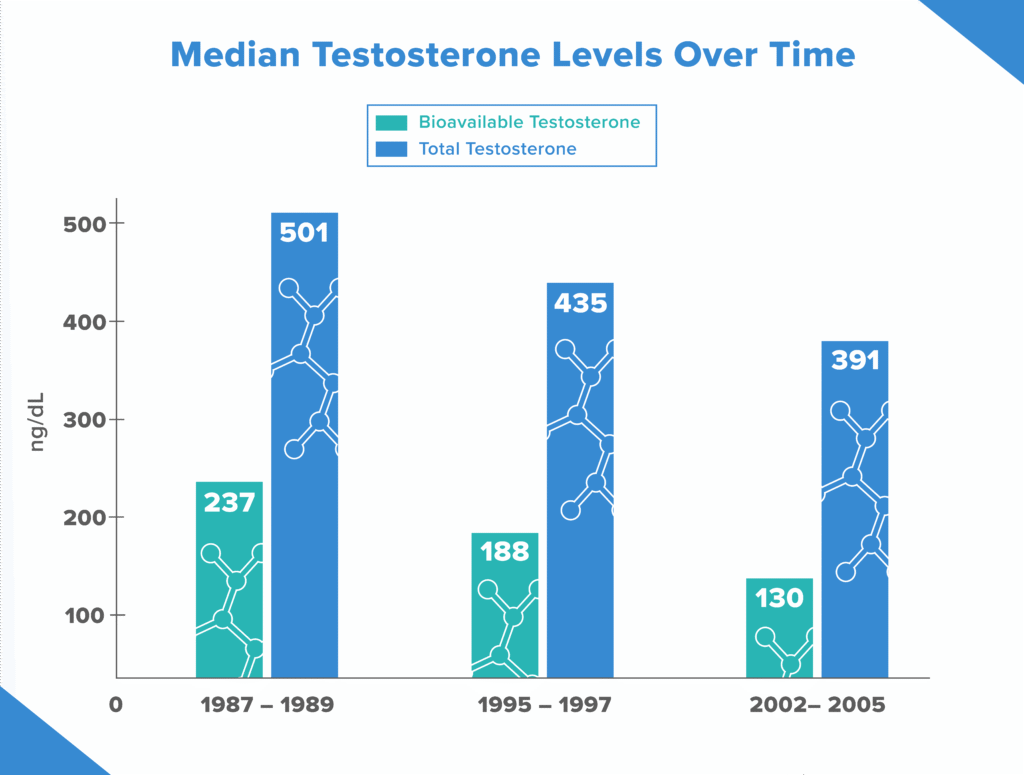
The average levels of the male hormone dropped by 1 percent a year, Dr. Thomas Travison and colleagues from the New England Research Institutes in Watertown, Massachusetts, found. This means that, for example, a 65-year-old man in 2002 would have testosterone levels 15 percent lower than those of a 65-year-old in 1987. This also means that a greater proportion of men in 2002 would have had below-normal testosterone levels than in 1987.
Why Pellets?
- Patients prefer testosterone pellets over gels or injections for several reasons, primarily due to their superior convenience and their ability to provide stable, consistent hormone levels.
- Avoid hormone fluctuations: Unlike other methods, the hormone fluctuations that can cause side effects and inconsistent symptom relief.
- No peaks and troughs: Injections can cause “peaks and troughs” in hormone levels, leading to mood swings, energy crashes, and inconsistent relief. Pellets prevent these fluctuations by releasing testosterone gradually.
- Steady symptom relief: The stable availability of hormones provides a more consistent improvement in symptoms like fatigue, low libido, and mood issues.
- Fewer side effects: The steady release profile of pellets is associated with a lower risk of side effects linked to hormonal spikes, such as irritability and fluid retention.
- Reduced risk of hormone transfer: Unlike gels or creams, pellets are implanted under the skin, so there is no risk of accidental transfer to others.
- Long Duration of treatment: Pellets are typical placed every 3 months in women and every four months in men.